Best Practice: Ear Cleaning Maximizes Successful Treatment of Otitis Externa in Dogs
James Owen Noxon, DVM, DACVIM (SAIM)

This content is provided by Blue Buffalo and has been peer reviewed. Clinician's Brief does not inherently endorse any product or organization advertised across its properties. The appearance of an advertisement on Clinician's Brief properties is neither a guarantee nor an endorsement of the product or advertising claims. Clinician's Brief is not responsible for the content promoted in an advertisement.
The “Best Practices” of veterinary care for patients presenting with otitis externa include: 1) Perform appropriate diagnostics, 2) Properly prepare the canal for treatment, 3) Choose ear medications wisely, 4) Apply medications properly (dose, frequency, methods, duration of therapy), 5) Perform quality control by rechecking the patient with appropriate diagnostics at an appropriate interval, 6) Provide maintenance therapy for patients with chronic or recurring otitis, and 7) Identify and control all factors of otitis (primary, secondary, perpetuating and predisposing). Ultimately, cleaning the ears affects all of these best practices and is the key step in “preparing the ear canal for treatment”. (Nuttall 2004)
JUSTIFICATION AND INDICATIONS FOR EAR CLEANING
Ear cleaning is indicated to facilitate treatment in almost all cases of otitis externa, even when the ears appear to be relatively clean. Ideally, ears should be cleaned prior to instilling medications when any exudate is present and it is critical to clean if debris obstructs a full view of the tympanum. A reminder that all relevant diagnostic samples should be collected prior to cleaning!
Cleaning the ears accomplishes the following:
Cleaning removes debris that may cause irritation. This includes foreign objects, some parasites, and wax, which can cause inflammation and irritation with excessive or prolonged contact in the canal. In vitro studies have clearly shown that most antimicrobials do not penetrate canine cerumen (i.e., ear wax) effectively, which may prevent the active drug from reaching the point of infection. (Stahl 2013)
Cleaning removes hair and debris (e.g., wax) that may block the movement of medications into the proximal ear canal. Hair can effectively block movement of debris (i.e., wax, exudate) out of the canal, thus interfering with self-cleansing” mechanisms of the ear, and equally importantly, it clearly prevents some medications from moving deep into the proximal, horizontal canal. We do not recommend traction to pull hair from healthy ears, since we have seen several cases with flare-ups of otitis caused by trauma following grooming episodes. However, if otitis is present, we strongly encourage careful removal of hair to allow for effective treatment!
Cleaning reduces the microbiological “burden” in the ear canal by physically removing large numbers of infectious agents. Starting treatment with a lower burden of infectious agents will very likely result in fewer residual infectious agents at the end of treatment.
Cleaning removes debris (including pus, wax, and biofilm) that interferes with activity of the active ingredients of otic medications.
EAR CLEANING SOLUTIONS
There are numerous commercial ear cleaning solutions available to the veterinarian. While there are numerous in-vitro studies investigating key properties of cleansers, patient directed comparative studies (in vivo) performed in laboratory animals or clinical patients are sparce. When the otitis is ceruminous (heavy wax buildup), better cerumenolytic activity may be achieved using products such as Cerumene® (Schering-Plough Animal Health), DUOXO® Micellar Ear Cleanser (CEVA), or pHnotix (Vetoquinol). (Nielloud 2019, Sanchez-Leal 2006, Marignac 2019) Alternatively, installation of a cerumenolytic agent or products containing squalene, are best used by instilling product in the ears and allowing it to sit for 5-20 minutes, followed by cleaning with an otic cleanser.
There have been numerous in vitro studies that demonstrate antimicrobial activity against Staphylococcus intermedius, Pseudomonas aeruginosa, and Malassezia pachydermatis by several commercial cleansers. (Lloyd 2000, Steen 2012, Swinney 2008) These studies vary greatly in their methodology and vary in contact times, application methods, and interpretations of data. Cleansers appear to be more effective when the offending organism is Malassezia spp. yeast. (Mason 2013) Limited numbers of patient directed studies evaluating antimicrobial effectiveness do also show some success in treating infections using only otic cleansers, but again, the methodologies and interpretations are highly variable. (Bassett 2004, Reme 2006) Most cleansers contain an antiseptic of some type, such as chlorhexidine, and some contain antifungal agents, such as ketoconazole; however, the specific antimicrobial agents vary from product to product. Overall, studies strongly support the value in cleaning ears in dogs with infectious otitis. Intermittent use of ear cleansing agents with antimicrobial activity may also be sufficient for long-term maintenance/prevention of otitis externa.
EAR CLEANING METHODS
Manual Removal of Wax/Debris
Foreign bodies, parasites, and waxy debris (including ceruminoliths) may be removed manually using alligator (or other) forceps, cotton swabs, curettes, or ear loops. These instruments can be very effective and are best used in an anesthetized patient, since sudden movement can result in trauma to the canal, the instrument (breakage), or the tympanic membrane. There is a steep learning curve with these instruments. Inexperienced users often traumatize the tympanic membrane due to the lack of depth perception caused by working in a long, narrow canal. However, with practice and good technique, ears can be effectively cleaned with these instruments.
Hand-Cleaning
Perhaps the most commonly employed method of ear cleaning by veterinary practitioners is hand cleaning or flushing of the ear canals. This is performed by filling the canal with an ear cleanser and then gently massaging the canal externally to break down adherent debris in the canal and facilitate absorption / movement into a cotton ball placed in the opening of the canal. The process should be repeated multiple times until material that is massaged out of the canal is no longer discolored and no longer contains chunks of waxy debris.
Bulb Syringes
A bulb syringe is a hollow rubber sphere with an adjoined tapering nozzle. Cleaning solution may be sucked up into the sphere and then the nozzle placed in the ear canal and fluid flushed back and forth into the canal and back up into the sphere. This creates turbulence which can be very effective at breaking down debris and facilitating removal. However, the nozzle is tapered and placement too deep into the canal can result in a seal of the nozzle and canal, in which case damage (i.e., rupture) to the tympanic membrane can result from the pressure or vacuum created by process. The author does not recommend use of bulb syringes by pet owners and recommends their use by veterinary personnel only with great care with the patient under sedation.
Deep Ear Cleaning (Flushing)
Deep ear cleaning is indicated when the tympanic membrane is not visible through routine diagnostics. It should be performed with the patient under general anesthesia. Heavy sedation is usually not adequate due to the sensitivity of the proximal ear canal/tympanum and the likelihood that some surgical procedure will be indicated once complete inspection of the canal is performed. The procedure may be done through hand-held manual otoscopes or a video-otoscope, though the latter device definitely improves visualization of the canal and is highly recommended.
Three flushing devices have also been developed and manufactured for use in conjunction with video-otoscopes employ combination suction and flushing through a hand-held device that can fit through the channel on a video-otoscope or through an operating head of a manual otoscope. These devices can be effective for ear cleaning; however, techniques described below are equally effective.
The author’s preferred method employs a three-way stopcock connected to two intravenous extension sets: one runs to a catheter (tomcat style, feeding tube, or polyethylene urinary catheter that has been trimmed to an appropriate length) and the other connected to a 30 ml syringe in which body temperature sterile saline will be used to flush the canal. The third point on the stopcock is connected to a suction device. An assistant will be required to manipulate the stopcock between flushing and suction, to flush the sterile saline using pulsating pressure on the syringe, refilling syringes as needed.
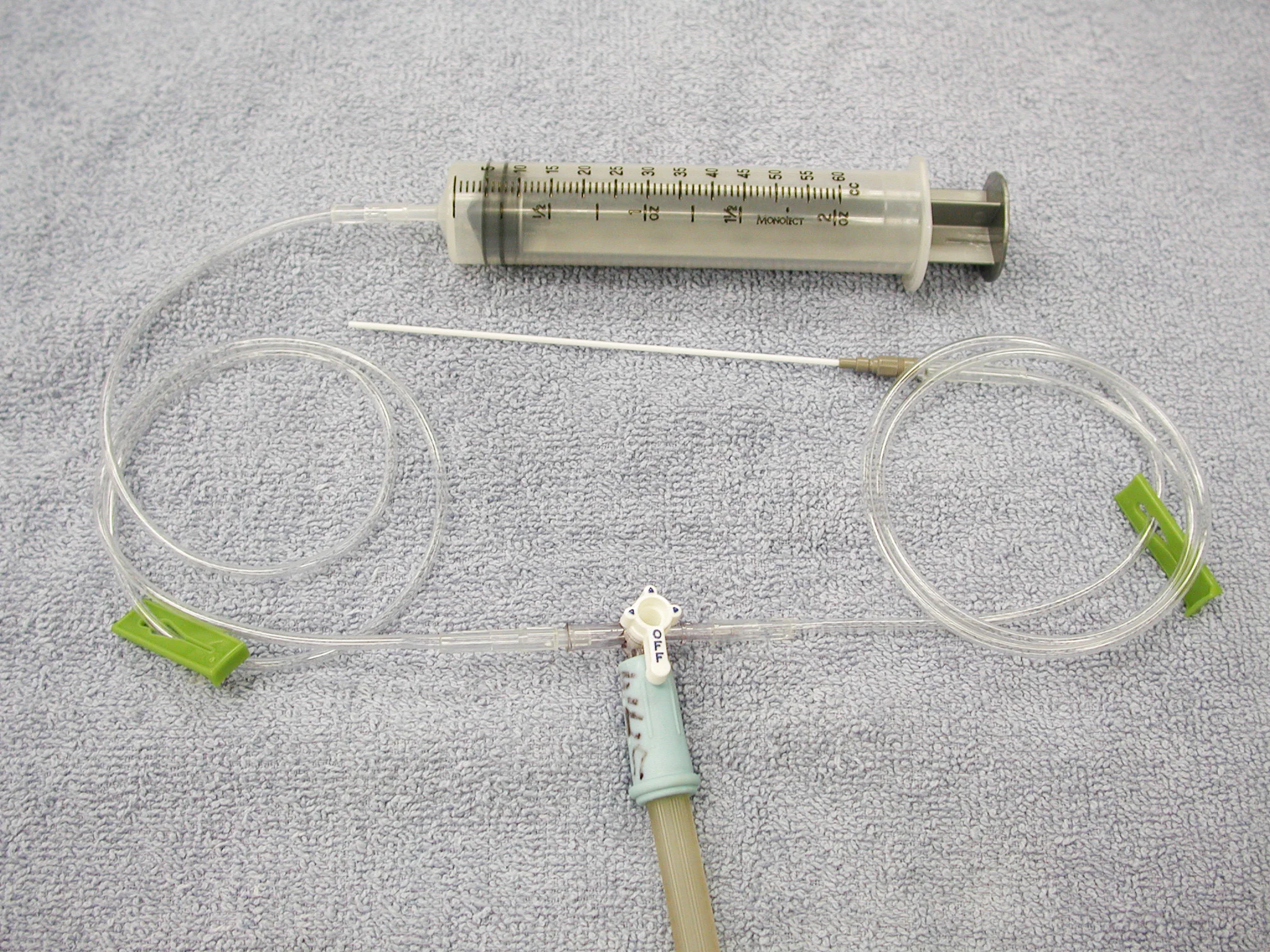
Setup of catheters and extension set for deep ear flushing
Deep ear cleaning is more effective after the ear has been instilled with a cerumenolytic agent, especially those containing squalene. The ear should be flushed to remove all traces of exudate and debris. Care is always taken to avoid traumatizing the canal or tympanic membrane. This same technique is used to flush the middle ear, when necessary. If there is any question about the integrity of the tympanic membrane, the patient should be intubated and the cuff carefully inflated prior to deep ear flushing, since fluid could gain access to the pharynx through the auditory tube.
Following flushing, appropriate mediations, such as n-acetylcysteine, iodine, Tris-EDTA, and specific otic medications, may be directly placed deep into the canal to ensure complete coverage of the surface of the canal.
FREQUENCY OF EAR CLEANING
There is great variety about the recommended frequency of ear cleaning by owners and veterinarians in the literature. The author does not recommend cleaning of pet ears by the owners because 1) the efficacy of owner cleaning is tremendously variable and often completely ineffective, 2) over aggressive owners may cause additional physical damage to the canal or tympanic membrane, and 3) over-cleaning may cause maceration or infection. One study showed that up to 17% of ear cleaner samples collected from canine pet owners who cleaned ears routinely were contaminated with bacteria. (Bartlett 2011) The contamination rate varied with the bottle size, ingredients, and dates of expiration.
This author recommends ear cleaning by the veterinarian or technician at the time the diagnosis of otitis is initially made, especially if the integrity of the tympanic membrane cannot be determined. Repeated cleanings are not necessary in most cases, until a recheck examination at 2-3 weeks. In some cases where there is a recurring large amount of ceruminous material, owners may be carefully instructed on ear cleaning techniques for routine home cleanings at a maximum frequency of once weekly.
The value of ear cleaning to maximize treatment of otitis is demonstrated by a recent study of dogs with chronic Malassezia otitis with a median duration of otitis of 9 months. Following referral and a single ear flushing done with a video-otoscope, the otitis was treated successfully in 88% of the ears (n=60) regardless of the otic medications used for follow-up treatment. (Boone 2021) In addition, a recent survey showed that treatment of chronic otitis externa by specialists was more successful when treated by a primary care veterinarian. The main difference in treatment was increased use of glucocorticoids and higher rate (55% vs 3%) of deep ear cleanings done by specialists. (Logas 2021)
Cleaning does maximize success in the management of canine otitis externa.