Canine Pelvic Limb Amputation
James Howard, DVM, MS, DACVS, The Ohio State University
Kristen French-Kim, DVM, The Ohio State University
Stephen C. Jones, MVB, MS, DACVS-SA, The Ohio State University
Nina R. Kieves, DVM, DACVS-SA, DACVSMR, CCRT, The Ohio State University
Discussion
Pelvic limb amputations are palliative salvage procedures used for end-stage diseases, including complex fractures or chronic complications with previous repairs, appendicular neoplasia, extensive trauma, chronic nonhealing wounds, or appendicular neuropathies (eg, brachial plexus avulsion). Some amputations are necessary due to the pet owner’s financial constraints. However, surgeons are encouraged to exhaust all options prior to limb amputation while also educating owners about the risks, complications, and prognosis for each specific clinical case.
The midfemoral amputation technique protects male genitalia with favorable cosmesis but can cause a greater likelihood of muscle atrophy and pressure sores. Amputation by coxofemoral joint disarticulation, however, obviates the risk for delayed muscle atrophy and has favorable cosmesis. This procedure provides a predictable outcome and reduces the likelihood of pressure sore development, thereby improving postoperative recovery and at-home incision management as compared with the midfemoral technique.
Complete presurgical orthopedic and neurologic examinations are necessary. Dogs undergoing pelvic limb amputation adapt through increased tarsal range of motion in the contralateral limb, coupled with increased range of motion of the cervicothoracic and thoracolumbar vertebrae.1 It is important to explain to owners that, although amputations typically have a good prognosis, increased BCS negatively correlates with quality-of-life scores.2 Preoperative surgical preparation varies based on patient size, although the landmarks used are identical regardless of patient size (see Step 1). Owners should be informed that extensive removal of the patient’s hair coat prior to surgery is necessary and that regrowth will take some time.
Preoperative antibiotics (eg, cefazolin [22 mg/kg IV], ampicillin/sulbactam [30 mg/kg IV]) should be routinely administered at induction and every 90 minutes during surgery. However, because routine amputations are classified as clean procedures, postoperative antimicrobial stewardship should be considered before continuing antibiotics. In most cases, unless there is noticeable pyoderma surrounding the incision site, antibiotics are not necessary postoperatively. Preoperative epidurals, intraoperative perineural injections, liposomal encapsulated bupivacaine during closure, and/or placement of an indwelling pain-soaker catheter in the superficial tissues should be considered. Perioperative analgesics are necessary. Additional IV and oral analgesics should be administered during the postoperative period for 10 to 14 days depending on the patient’s comfort level. Injectable opioids (eg, morphine, methadone, fentanyl) can be administered immediately following surgery and later (next day following pain assessment) transitioned to oral NSAIDs for the duration of the recovery period.
Routine postoperative exercise restriction and incision care, including use of cold and warm compresses, are standard. NSAIDs, ancillary analgesics, and anxiolytics are routinely provided for at-home care.
Step-by-Step: Pelvic Limb Amputation
What You Will Need
Soft tissue surgery pack, including Mayo scissors, Metzenbaum scissors, forceps, a variety of hemostats, and right-angle forceps (optional)
Electrocautery
± Hatt spoon
Monofilament suture (4-0 to 0, depending on patient size)
Polydioxanone suture for vessel ligation, muscle apposition, and deep subcutaneous closure (4-0 to 2-0)
Poliglecaprone 25 suture for superficial subcutaneous closure (4-0 to 3-0)
Nonabsorbable monofilament suture (eg, polybutester [4-0])
Local anesthetic for perineural injection (recommended doses should not be exceeded)
Ropivacaine (0.5% or 0.75%): 1-3 mg/kg (dogs) and 1-2 mg/kg (cats)
Bupivacaine (0.25% or 0.5%): 1-2 mg/kg (dogs) and 1 mg/kg (cats)
Syringes and needles for perineural injections (syringe size depends on recommended doses; a 25-gauge needle is recommended for perineural injections)
4 x 4 or 3 x 3 gauze sponges and laparotomy sponges to control hemorrhage
Step 1
Clip hair from the level of the umbilicus, dorsally 2 to 5 cm past dorsal midline, ventrally 5 cm past ventral midline, around the entire inguinal and abdominal region, circumferentially around the pelvic limb to the level of the hock, from the perineal region, and from the base of the tail. If the patient has evidence of current soft stool or diarrhea, use an anal purse string suture. Wrap the limb distal to the hock in sterile bandage material during draping, and place the patient in lateral recumbency with the affected limb upward and the limb draped routinely.

Step 2
To ensure adequate skin is available for closure, identify the lateral incision (dashed line), which begins at the level of the cranial flank fold and (in a gentle arc) reaches its most distal point approximately halfway down the length of the femur, meeting the caudal flank fold near the ischiatic tuberosity. Also, identify the medial incision (solid line), which mirrors the lateral incision but is slightly more proximal.

Step 3
Abduct the limb to begin the medial dissection. Using right-angle forceps, incise the subcutaneous tissue and underlying deep femoral fascia with a combination of sharp and blunt dissection. Approach the femoral triangle by palpating the medial aspect of the pelvic limb and feeling for a short, tight muscular band (ie, the pectineus muscle).
Author Insight
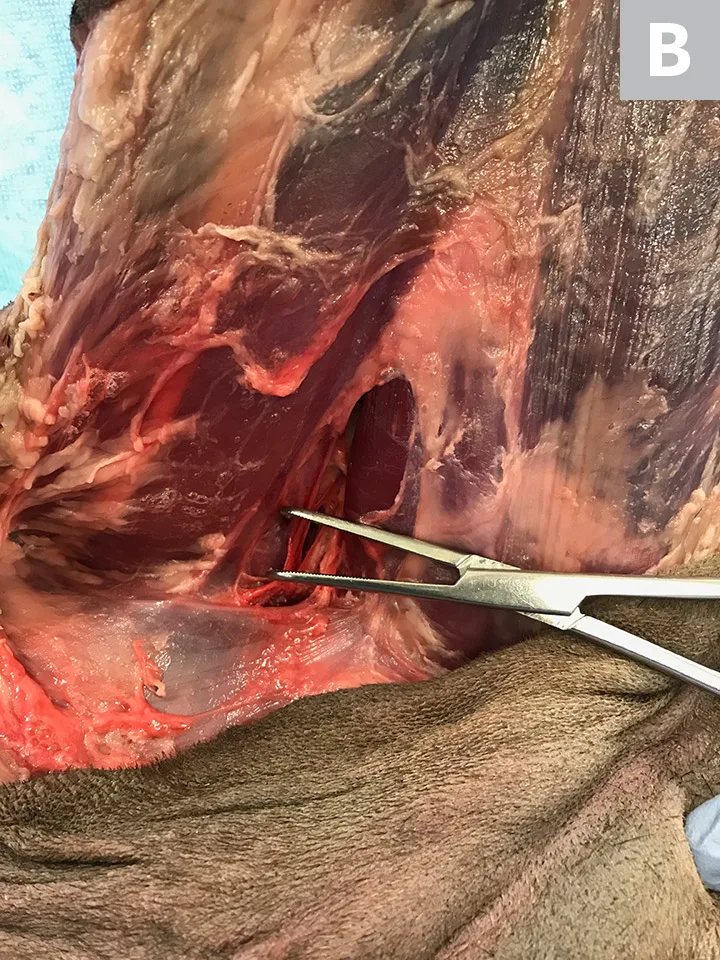
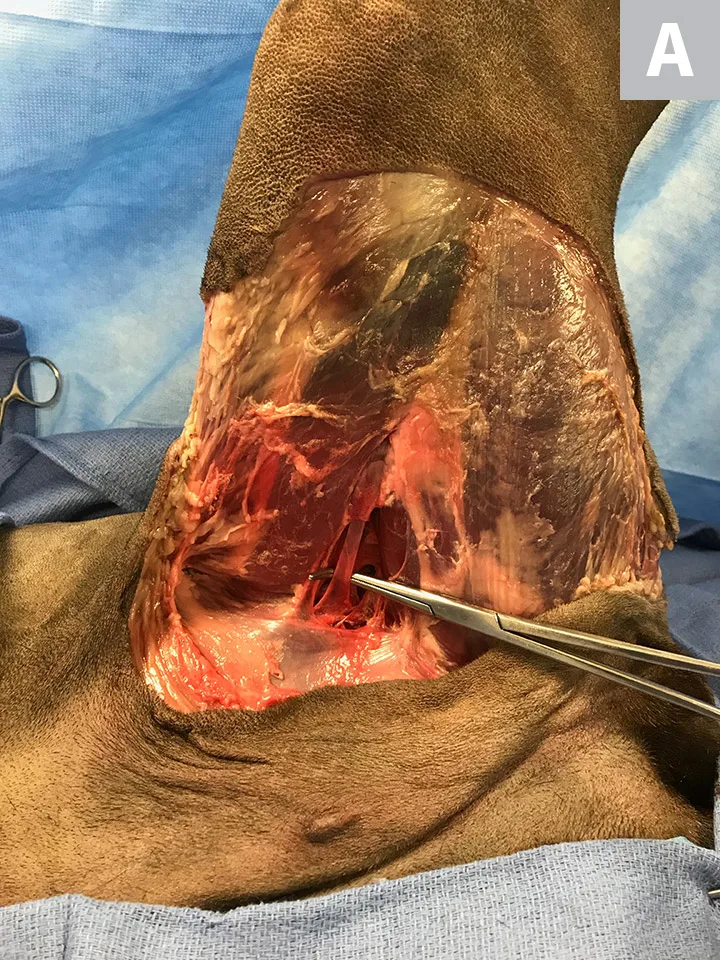
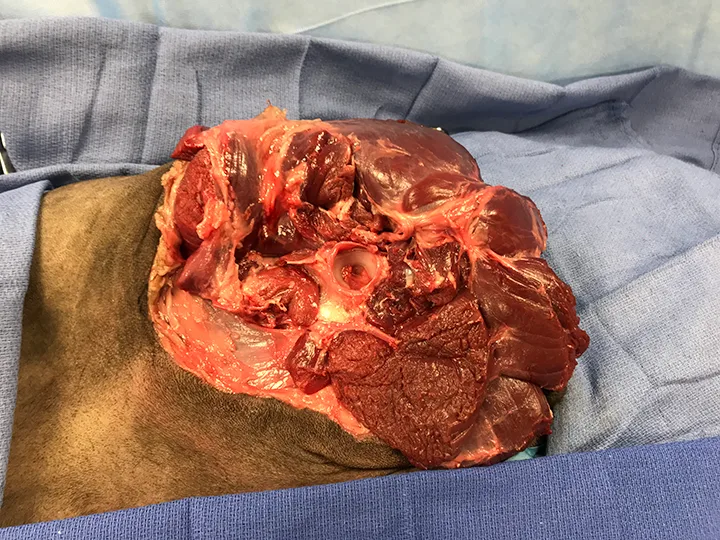
The femoral triangle provides passage of the femoral artery, femoral vein (Figure A; solid arrow), and saphenous branch of the femoral nerve to the pelvic limb. When dissecting vessels, blunt dissection using right-angle forceps should be used in a parallel orientation to the long axis of the vasculature (Figure B). This technique reduces the risk for accidental vessel rupture or penetration.
Boundaries of the femoral triangle are:
Cranial: Caudal sartorius muscle
Caudal: Pectineus muscle; easiest to palpate to find the triangle (Figure A; dashed arrow)
Lateral: Vastus medialis, pectineus, and iliopsoas muscle
Medial: External abdominal oblique muscle

Step 4
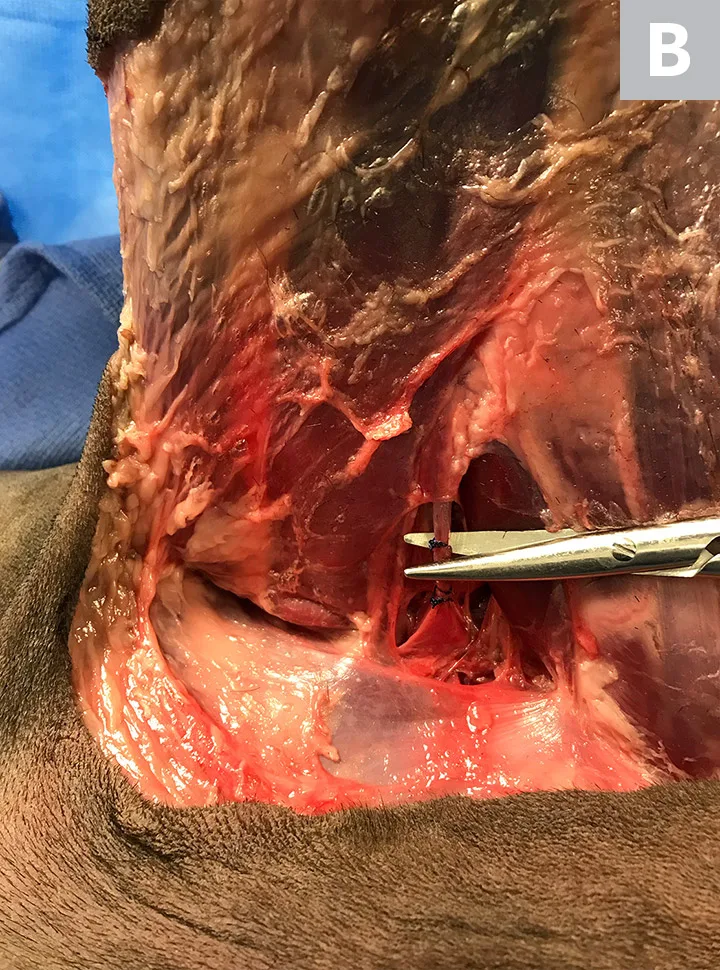
Dissect the femoral artery, vein (Figure A), and saphenous branch of the femoral nerve. Triple ligate each vessel. Place a single transfixing and circumferential suture on the side of the vessel that will remain with the patient, then place another single circumferential suture on the side of the vessel that will remain with the amputated limb to prevent back-bleeding. Transect the vessels between the transfixing suture that will stay with the patient and the circumferential suture that will prevent back-bleeding (Figure B). To provide local nerve blocks, insert the needle into the perineural sheath and inject a small amount of ropivacaine or bupivacaine. A small “bleb” will form. Wait 3 minutes, then transect the nerve distal to the injection site.
Author Insight
Large arteries and veins should always be ligated with a transfixing suture and 2 circumferential sutures. This is common practice in medium to large dogs. Arteries and veins in small dogs and cats can be ligated with 3 circumferential sutures only; 2 sutures always stay with the patient side of the vessel and one will be removed with the amputated limb to prevent back-bleeding.
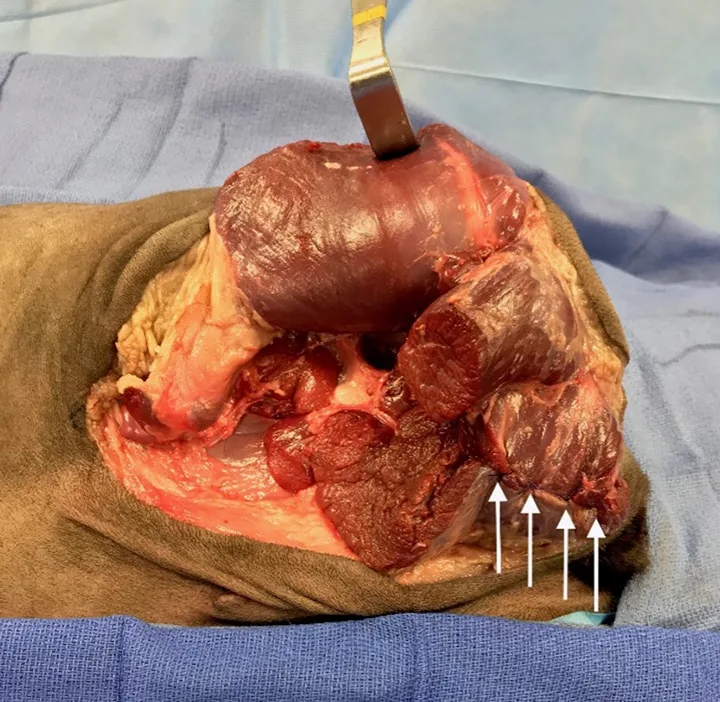
Step 5
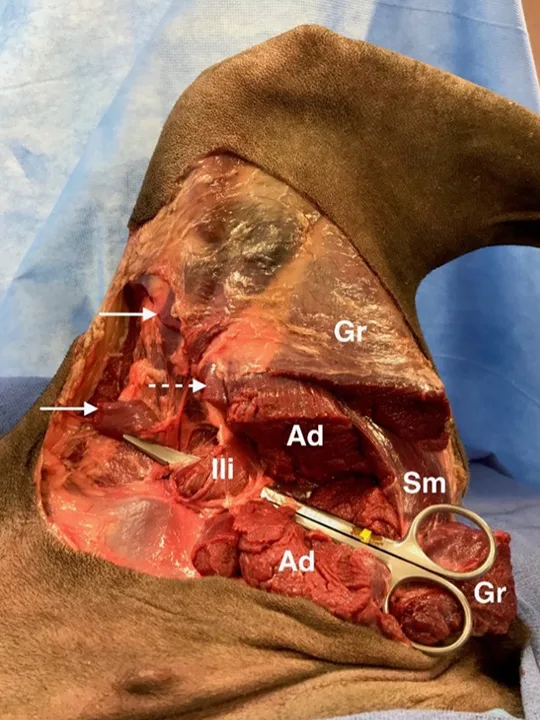
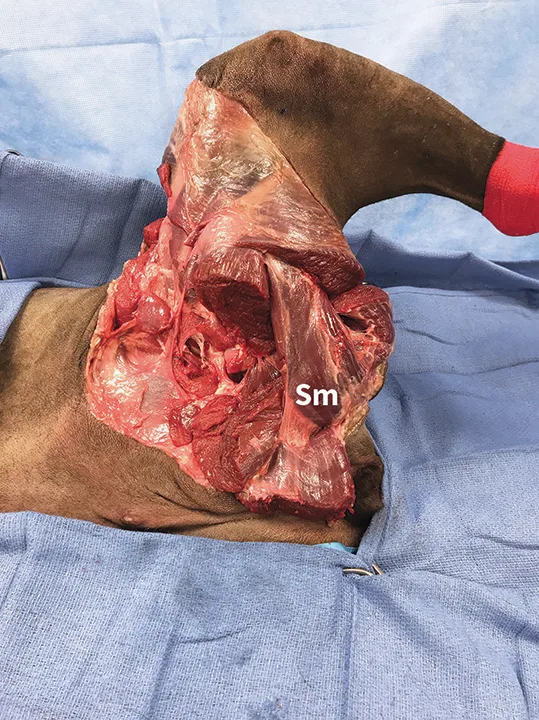
Work cranially and caudally to transect the cranial and caudal bellies of the sartorius (solid arrows), pectineus (dashed arrow; this can be transected at its origin, midbelly, or insertion), adductor (Ad), and gracilis (Gr) muscles midfemur. Once the medial circumflex femoral artery and vein or the deep branch of the medial circumflex femoral artery and vein* are encountered, ligate using the same technique described in Step 4. (The semimembranosus [Sm] is labeled for orientation.)
Palpate the lesser trochanter of the femur, then transect the iliopsoas (Ili) midbelly or at its insertion.
Author Insight
Only the extrinsic pelvic limb muscles (ie, those that attach the limb to the pelvis) need to be transected. Excessive dissection of the quadricep muscles can prolong surgical time and increase the risk for complications.
The femoral nerve courses through the iliopsoas muscle before exiting the muscle belly and penetrating the rectus femoris and vastus medialis. The femoral nerve can be injected with ropivacaine or bupivacaine and transected.
*The vascular bundle is located caudal to the femoral artery and vein, medial to the pectineus muscle, and lateral to the iliopsoas [Ili] muscle.
Step 6
Palpate the medial joint capsule (dashed arrow), and sharply incise into it following the anatomy of the acetabular cup. Once the joint capsule is open, disrupt the ligament of the head of the femur with a scalpel blade, Mayo scissors, or Hatt spoon. (The iliopsoas [Ili] muscle is identified with the solid arrow for orientation.)

Author Insight
The limb should be put through range of motion to isolate the coxofemoral joint to guide the incision into the joint capsule.
Step 7
Adduct the limb for the lateral aspect of the muscular attachments. Transect the tensor fasciae latae (TFL) muscle at its distal aspect and the associated fascia lata (FL) near midfemur. In the same plane of dissection, transect the biceps femoris (BF) and caudal crural adductor (CCA) near the level of the midfemur. Do not transect the sciatic nerve, which is deep in the muscles, prior to injecting local anesthetic, as unnecessary neuropathic postoperative pain can cause patient discomfort.
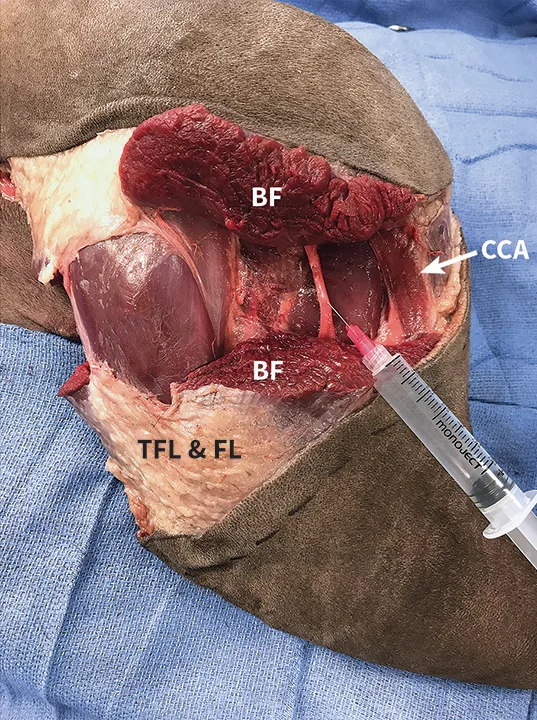
Author Insight
The biceps femoris arises from the ventrocaudal aspect of the sacrotuberous ligament and ischial tuberosity, allowing the proximal portion of the transected muscle belly to reflect dorsally, thus facilitating dissection and midbelly transection of the semitendinosus (St) and semimembranosus (Sm) muscles.
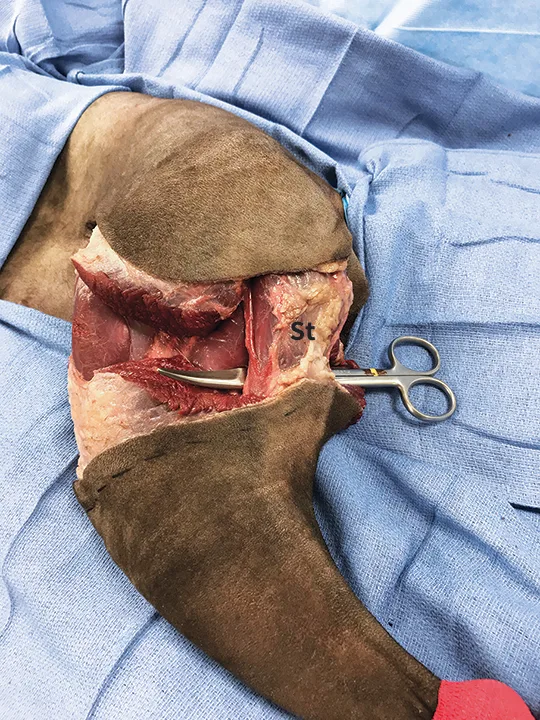
Step 8
As the dorsal reflection of the biceps femoris muscle exposes the greater and third trochanteric region of the femur (improving visualization of the superficial, middle, deep gluteal, and deeper piriformis muscle insertion sites), transect each close to its insertion.
Reflect the superficial gluteal and piriformis muscles dorsally, and bluntly dissect the underlying fascia to isolate the caudal gluteal artery, vein, and sciatic nerve (previously transected) that are adjacent to each another. Triple ligate the caudal artery and vein separately.
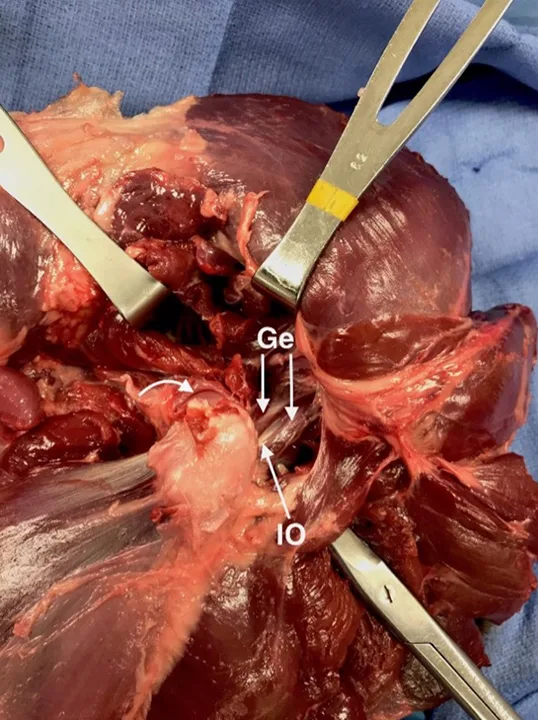
Step 9
At the caudal aspect of the hip, locate the gemelli (Ge) muscles; the bellies are bisected by the tendon of the internal obturator (IO) muscle. Transect the gemelli muscles midbelly along with the tendon of the internal obturator muscle.
Dorsally and ventrally reflect the gemelli muscle bellies to expose the underlying external obturator muscle, then transect it midbelly. Simultaneously transect only the rectus femoris, as it is the only muscle of the quadriceps group attached to the pelvis.
At the dorsal aspect of the acetabulum, incise the remaining portion of the joint capsule (curved arrow) with the small articularis coxae muscle. Ligate the underlying branch of the lateral circumflex femoral artery.
At the caudal aspect of the limb, isolate the abductor cruris caudalis (scissors under muscle in image), and transect it midbelly.
Step 10
Identify the iliopsoas muscle by its close proximity to the parent femoral nerve. If the saphenous branch of the femoral nerve has not already been transected, transect the parent femoral nerve. To free the cranial and ventromedial aspect of the limb, abduct the limb, transect any remaining iliopsoas muscle attachments, and ligate any remaining branches of the medial circumflex femoral vessels.
Caudal to the iliopsoas muscle, isolate the adductor longus and quadratus femoris muscles, and transect each muscle at midbelly.
Complete the ventral incision into the joint capsule. Use monopolar electrocautery to maintain hemostasis.
Gently abduct the limb to expose the head of the femur. Transect any remnants of the ligament of the head of the femur to complete the coxofemoral disarticulation. Remove the limb from the body.
Author Insight
Smaller branches of the medial circumflex femoral artery are in close proximity to the ventral aspect of the joint capsule.
Step 11
Prior to closure, inspect the surgical field for bleeding and plan to prevent dead space. Lavage the surgical field with warm saline to minimize the potential for postoperative infection.
Step 12
Start deep muscle closure. Appose the muscle bellies to protect the acetabulum and the transected ends of the femoral artery, vein, and nerve. Use either a continuous or interrupted suture pattern (arrows) with absorbable suture material (suture size, 3-0 to 0, depending on patient size).
Step 13
Close the subcutaneous tissue layer routinely. If desired, place an indwelling pain-soaker catheter in the superficial tissues for postoperative administration of local analgesics—do not place in the closure of the incision. Triangular protrusions of skin (ie, “dog ears”) may form at the termination of the suture lines. If there is excessive skin in this area, it can be removed and closed routinely. Smaller “dog ears” can be corrected with multiple geometric correction techniques including placement of an apex cutaneous suture, removing the dog ear with a fusiform shape extending from the original incision, or removing a triangular-shaped portion of skin extending from the incision, among others.
Author Insight
Throughout closure, care must be taken to ensure there is enough skin for closure. Any excess skin should be excised to prevent excess dead space.
Step 14
Perform skin or intradermal closure using either a continuous or interrupted pattern (suture size range, 4-0 to 3-0, depending on patient size).

Author Insight
Staples are not recommended due to discomfort and increased inflammation but may be considered with longer incisions in larger dogs.