The Latest Advancement in Veterinary Airway Management
Ivan Crotaz, MRCVS
Sponsored by Jorgensen Laboratories
Airway management devices connect the anesthetic circuit to the respiratory system of patients. These devices have various functions, including protecting against aspiration, providing the anesthetist control over respiratory depth and rate, and movement of anesthetic, respiratory, and waste gases.
In human anesthesia, many different airway devices are available. Until the launch of the species-specific supraglottic airway device, v-gel®, veterinary surgeons only had 2 options to manage an airway during anesthesia: endotracheal tube or face mask. The introduction of v-gel® provided veterinarians with a low trauma, wide diameter airway that was easy to place.
The latest v-gel® product, v-gel® Advanced, has widened the scope of these devices for general practice anesthesia, dental anesthesia, and specialist anesthesia. This article will review the pros and cons of the 3 airway management methods and experiences with v-gel® Advanced.
Face Mask
Face masks allow patients to breathe in an oxygen-rich gas mixture. Care must be taken to not press the nostrils against the mask wall, as this will obstruct the airway. Mask seals should be positioned away from the eye. Corneal ulceration is a possible complication of mask use, especially in rabbits and brachycephalic cats.1
Face masks are effective for oxygen supplementation but can be difficult to seal around the nose and mouth of veterinary species and are unlikely to have a good gas seal. When gaseous anesthetic agents are used, environmental contamination is almost unavoidable,2 which presents a significant health and safety risk. Specialist double (scavenging) masks are used in laboratory animal medicine to reduce this risk but do not eliminate environmental contamination.
Face masks increase total dead space (the volume of gas that must be moved before the patient can access fresh gas flow). This can be highly significant in small patients such as rabbits. Exhaled CO2 mixes with incoming fresh gas within the mask, leading to some of the exhaled CO2 being re-inhaled. Using the smallest possible face mask can help minimize this rebreathing effect.
Face masks are effective for oxygen supplementation but can be difficult to seal around the nose and mouth of veterinary species and are unlikely to have a good gas seal.
The author uses face masks purely for oxygen supplementation in sedated patients or during extremely short procedures. Ventilation is possible but can lead to environmental contamination if anesthetic gases are being used. Face masks also do not offer protection against fluid aspiration or anatomic airway obstruction.
Endotracheal Tube
Most veterinarians are familiar with endotracheal tubes, which are inserted through the mouth, then between the arytenoid cartilages of the larynx and into the trachea. Nasotracheal tube placement is also sometimes used.3
There are common issues associated with endotracheal tubes that create morbidity and are difficult to protect against. Endotracheal tubes rest on the inner surface of the larynx and trachea, which creates mucosal trauma.4 Cats in particular are sensitive to laryngospasm as a result of intubation.5 Excessive cuff inflation can cause direct tracheal rupture or reduce mucosal vascular supply, causing tracheal necrosis and delayed tracheal rupture.6
The cuff of an endotracheal tube is not the barrier to aspiration that is commonly imagined. Cuffs are a partial aid to airway protection, not an absolute one; folds in the inflated cuff surface allow fluid to track past the cuff into the lower airway.7 Use of pharyngeal sponges or swabs can reduce the risk for aspiration associated with regurgitation. If these are used, it is vital for the recovery checklist to include removal of the swab or sponge before the tube is removed.
Endotracheal tubes narrow the airway of patients. This can be useful in human anesthesia, in which ventilation is normally used because it reduces anatomic dead space; however, this can present problems in veterinary anesthesia, in which it is uncommon to assist the patient with the work of breathing. Small reductions in airway diameter can lead to huge increases in airway resistance (Figure 1).
v-gel® Advanced Supraglottic Airway Device
v-gel® veterinary supraglottic airway devices are anatomically shaped products that are positioned dorsal to and surrounding the larynx and epiglottis. The proximal end of the device rests within the proximal oesophagus to stabilize the device and help hold any regurgitated fluid away from the airway. By sealing proximal to the larynx, they allow the full width of the anatomic airway to be utilized.
The original v-gel® devices were designed to allow the clinician to maintain a wide airway, without touching and potentially traumatizing the larynx and trachea. These devices were easy to insert and produced less stridor (upper respiratory noise) in the anesthetic recovery period than an endotracheal tube.8
In the author’s experience, v-gel® devices made rabbit anesthesia considerably easier. It became possible to obtain an airway within seconds and monitor respiratory function throughout anesthesia. Recovery was smoother than with other airway devices, with fewer postanaesthetic appetite problems. Using v-gel® devices allowed clinicians to reduce anesthetic-related morbidity (eg, pain, laryngeal spasm, issues related to airway resistance) while simultaneously making airway access easier and faster, especially in emergencies.
v-gel® Advanced devices (Figures 2 & 3) were produced in response to the clinician’s need for better airway seals for ventilation and for superior access for dental procedures while retaining the advantages of the original devices.
Using v-gel® devices allowed clinicians to reduce anesthetic-related morbidity (eg, pain, laryngeal spasm, issues related to airway resistance) while simultaneously making airway access easier and faster, especially in emergencies.
The v-gel® Advanced device uses a flexible wall seal that wraps around the larynx and epiglottis (Figures 4 & 5) and seals against the floor of the pharynx. The oral section has been re-engineered to be much more streamlined but just as strong as the original version. In the author’s experience, v-gel® Advanced seal pressures are in the region of 15-25 cmH20 in both cats and rabbits. This works well for both manual intermittent positive-pressure ventilation (IPPV) and mechanical ventilation. The v-gel® Advanced device does not have an inflatable cuff; the seal is the result of fitting the flexible device into the correct position. The author routinely uses v-gel® Advanced devices with a mechanical ventilator in rabbits, which allows for easy management of hypercapnia, a common yet serious and potentially fatal complication of anesthesia in rabbits.
An advantage of this encompassing seal is a double layer of protection against aspirated fluid. The distal oesophageal tip offers resistance to oesophageal fluid, working with the slim seal (Figures 6 & 7) surrounding the larynx and isolating it from the pharynx. Although no protection is absolute, the author has observed cases in which regurgitated fluid has been held away from the airway by this seal. It is critical to follow normal guidelines on preoperative feeding, gastroprotection, surgical positioning, protection from dental instrument cooling fluids, and use of protective swabs/sponges to increase fluid protection.
The wider size spectrum of the v-gel® Advanced, with smaller and larger devices added to the range, is especially useful in feline anesthesia (eg, in early neutering or with very large breed cats). Because of the risk for endotracheal tube-associated laryngospasm,9 the v-gel® Advanced device is the author’s choice for routine feline and dental anesthesia (Figure 8). For clinicians used to the original v-gel® device, the v-gel® Advanced device is easy to switch to, with the same insertion, monitoring, and removal rules. Instructions for use are available at docsinnovent.com/information-sheets.
The smaller size of the oral section of the v-gel® Advanced dramatically improves dental surgical access as compared with the original v-gel® (Figure 9). The oral section can be moved without displacing the pharyngeal section to make access even easier.
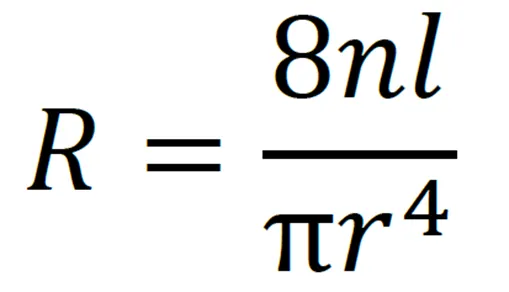
FIGURE 1
Poiseuille’s law. Resistance (R) is inversely proportional to the tube radius (r), where n equals the viscosity of the substance (anesthetic gas in this case) and l the length of the tube. Assuming there is laminar flow within an endotracheal tube, halving the radius of the tube increases the resistance to flow by 16 times.
It is important that v-gel® Advanced be inserted under a surgical plane of anesthesia. The seal edge is taller than that of the original v-gel®; if patients tense up during insertion, the seal will not reach the right position and the device may be less effective. Most of the complications that the author has encountered with the Advanced device relate to placement in insufficiently anesthetised animals, particularly rabbits. A controlled IV anesthetic induction allows for easy adjustment of anesthetic depth to make placement simple.
If the v-gel® device cannot be easily inserted into the pharynx, the patient may need a greater depth of anesthesia or, in some cases, a smaller device.
If the device is leaking during active ventilation, it should first be repositioned. In some cases, a larger device may be needed to increase seal pressure, but pushing a very large device into a small pharynx can collapse the flexible walls inwards, compromising the airway.
With v-gel®, it is simple to measure and monitor patency of the airway after placement. Gentle bagging immediately after insertion should allow for the chest to be inflated with minimal effort and no audible leak. Capnography can also help monitor placement and respiratory effectiveness. If a patent airway is not present after v-gel® insertion, it is vital to reposition or remove and reinsert the device. Accidental autoclave damage was a common problem with the original v-gel® device; however, this issue has been eliminated with the new single-use design, as has the risk for cross-contamination.
Conclusion
No airway management device is appropriate for every situation. Clinicians should focus on what they need the device to achieve and what complications they are protecting against. v-gel® Advanced devices allow for a wide, low-resistance airway to be maintained, with minimal risk for airway trauma. Their upgraded engineered design seals the airway as well as or better than a cuffed endotracheal tube without the adverse effects that an endotracheal tube can have on the tracheal lining.