
Tail amputations can be broadly categorized as therapeutic (eg, neoplasia, external trauma, repeated injuries, or self-trauma) or nontherapeutic (eg, tail docking).
Indications
Tumors of the skin (eg, mast cell tumor), soft tissue (eg, sarcoma), or bone (eg, osteosarcoma) can occur along the tail. Depending on the location, adequate margins can be achieved via tail amputation (ie, caudectomy). Primary excision of skin tumors on the tail may lead to tension along the closure and can increase the risk for a tourniquet effect or dehiscence. Tail amputation should be considered for any malignant skin tumors to achieve both adequate margins and tension-free closure.
Another common indication for tail amputation is repeated self-trauma (mostly seen in dogs) caused by hitting the distal tail, sometimes forcibly, on surrounding structures. These repeated incidents can create scar tissue and more friable skin and lead to increased risk for future trauma, bleeding, and a nonhealing wound. Tail amputation should be considered in recurrent cases in which conservative (eg, bandaging) or behavioral management does not allow the wound to heal or prevent recurrence. The goal for these cases is not to amputate the entire tail but to shorten it enough to preclude recurrent self-damage.
Tail trauma in hunting dogs has been described.1 Vehicular accidents can cause degloving wounds of the tail similar to appendicular trauma. Wounds can be sutured and closed in some cases, but if there is not enough skin to allow tension-free closure, tail amputation may be preferable.
Anatomy of the Tail
Tail vertebrae are surrounded by closely attached dorsal (sacrocaudalis dorsalis lateralis and medialis), ventral (sacrocaudalis ventralis lateralis and medialis), and lateral (intertransversarius dorsalis caudalis and intertransversarius ventralis caudalis) bulky muscles. The main blood supply can be found on both lateral sides of the tail (lateral caudal arteries), with smaller dorsal (dorsolateral caudal arteries) and ventral (median caudal and ventrolateral caudal arteries) arteries.
Complications
Complications of tail amputation include bleeding, dehiscence, and infection. Although infection and dehiscence are not common, they may necessitate revision of the amputation to a proximal level and require removal of more proximal coccygeal vertebrae. Bleeding in large dogs can be decreased with an intraoperative tourniquet, depending on its tightness. Temporary intermittent loosening of the tourniquet during surgery allows timely identification of vessels that can then be ligated (larger vessels) or electrocauterized. Alternatively, the tourniquet can be loosened prior to closure to check for appropriate hemostasis. A sterile, self-adhesive bandage can alternatively be placed over or adjacent to the intended incision site if there is enough proximal space. The bandage creates a tourniquet effect when applied tightly, and the incision can be extended into the bandaging. Judicious use of monopolar electrocautery when dissecting muscle off the bone and during muscle transection also decreases hemorrhage (aiding in identification of vessels) and can be used in addition to a tourniquet, especially in large-breed dogs. Individual hemostasis of vessels would still be needed.
Tension-free skin closure reduces the risk for postoperative dehiscence; removal of an additional vertebra can be considered if there is tension. Perioperative placement of an anal purse-string suture can reduce the risk for fecal contamination, as does placing surgery drapes to only include the tail in the surgical field; however, in higher amputations (ie, sacrococcygeal caudectomies), draping the tail base and perineum typically cannot be avoided. Placing tape in a visible place (eg, top of the patient's head) with a reminder that a purse string was placed helps in remembering to remove the purse string postoperatively.
Postoperative Concerns
Postoperative incontinence due to traction on the nerves is a concern with amputations at, or close to, the level of the sacrococcygeal junction. A small stump of several coccygeal vertebrae is ideally left to minimize the risk for incontinence; however, if the trauma or tumor are situated more proximally, care should be taken during dissection to avoid traction.
Although postoperative bandaging can protect the tail stump from self-trauma and keep it clean, bandages can slip easily and are often unnecessary. If a bandage is placed, care is needed to not attach the more proximal part too tightly, as a tourniquet effect is possible.
Step-by-Step: Therapeutic Tail Amputation
What You Will Need
IV stand (or similar) to hang the tail during preparation
Soft tissue surgical pack
Hypodermic needle
Electrocautery
4- × 4-inch gauze
Monofilament suture (based on patient size)
Polydioxanone sutures (or similar) for approximation of deeper tissue
Absorbable monofilament sutures for subcutaneous closure
External sutures (eg, nylon) or buried intradermal simple interrupted sutures (monofilament) for skin closure
Tourniquet (optional):
Penrose drain, IV tourniquet, or a rubber tie frequently used for endotracheal tube tie-ins
Sterile, self-adhesive bandage (alternatively)
Sterile marker pen to outline the incision and flaps (optional)
Sterile, self-adhesive bandaging if a wound or necrotic area needs to be covered (optional)
Purse-string suture to avoid contamination in a high tail amputation (optional)
Rongeurs to remove cartilage (optional)
Step 1
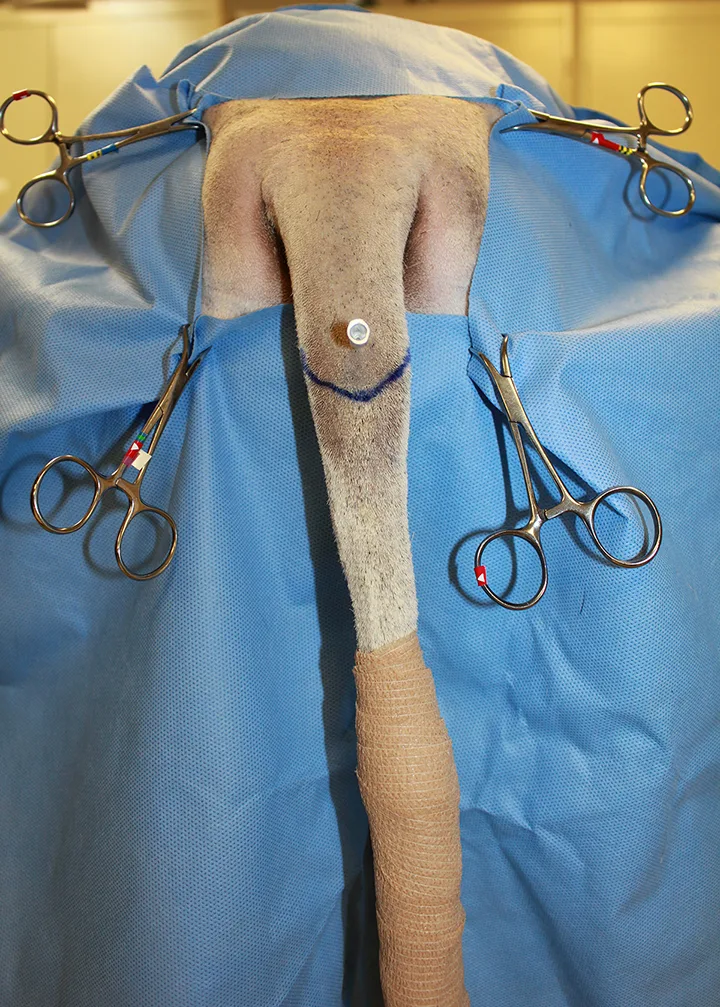
Clip the dorsal pelvic/lumbar area, tail, and perineum. Cover the most distal portion of the tail with a glove only, a glove covered with a second layer of self-adhering bandaging, or self-adhering bandaging only, as this part of the tail will be fully removed during surgery and does not need to be fully clipped. Place an anal purse-string suture. Position the patient in ventral recumbency and at the edge of the table, with the pelvic limbs hanging freely over the edge of the table (with an appropriate amount of padding underneath), or pull the patient forward with the pelvic limbs partially supported on the table. Suspend the tail to allow a hanging limb preparation and draping technique. Depending on the impermeability of the primary bandage, place a sterile self-adhering bandage (shown in Step 2) or an impermeable drape followed by a sterile self-adhering bandage to cover the distal portion of the tail and prepare for coverage.

Step 2
Choose the area of amputation and corresponding joint space. If desired, use a hypodermic needle to help identify the location of the intervertebral space. Place a tourniquet around the proximal aspect of the tail to decrease bleeding.
Author Insight
How long the tourniquet can be safely left in place depends on its tightness. Loosening and replacing the tourniquet every 20 to 30 minutes may be necessary.
Step 3
Plan to make the incision in 2 U-shaped flaps (ie, dorsal and ventral), with the tip of the U positioned toward the tip of the tail and the end of the “leg” of the U on the lateral side of the tail at the level of the planned disarticulation to allow for tension-free closure.

Step 4
Make an incision at the preplanned site, and dissect the subcutaneous tissue to the level of the desired disarticulation site (A). Reinsert the hypodermic needle at the desired intervertebral space after completing the subcutaneous dissection (B).


Step 5
Sharply transect the muscles of the tail, and dissect away from the intervertebral space. Maintain hemostasis of the arteries via targeted cautery or suture ligation of the arteries.


Author Insight
Transection can be done with monopolar electrocautery to minimize hemorrhage or with a blade (A). Here, a proximal ligature was placed in the vessel, and a hemostat was placed on the distal end (B). Suture tags were left long for illustrative purposes.
Step 6
Locate and disarticulate the joint space with a blade or heavy scissors. Remove the remaining cartilage at the proximal vertebra with rongeurs. Release the tourniquet prior to closure to check for hemostasis. Move and manipulate the skin to assess tension on the closure line before closing the wound.


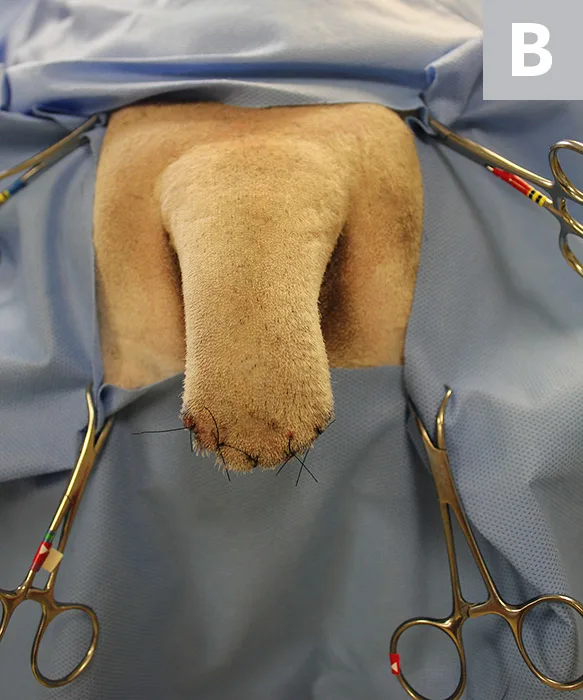
Step 7
Start closure by approximating sutures in the deeper tissues using a simple interrupted pattern (A), followed by routine closure of the subcutaneous tissues and skin (B). Trim the flaps if excess skin is present. After the incision is fully closed, remove the purse string (either in the operating room or in the preparation or recovery area).

Author Insight
Tail amputation without a tourniquet (especially for more distal amputations or in smaller patients) requires hemostasis in individual vessels as they are transected, rather than several at once after release of the tourniquet. A tourniquet can decrease bleeding, improve visualization, and be partially tightened in large dogs.